46 year old female patient with seizures
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan
NAME:- G VISHAL
ROLL NO :- 50
Patient was brought with complaints of 2 episodes of involuntary movements of upper and lower limbs and hemoptysis .
History of present illness :-
Patient was apparently asymptomatic then she developed sudden onset of movements of both upper and lower limbs at 5am in the morning which lasted for about 4-5mins , not associated with any trigger, no aura and the patient was confused after the episode
she had an other similar episode while she was brought to the hospital.
She had similar episodes at the hospital.
Sequence of events :-
13 years ago she developed low back ache and generalised weakness started for which she went to local hospital.
Then during the investigations was found to be having soft tissue overgrowth,(as said by attenders ,no documentation)and need to get operated, during routine investigations creatinine was elevated, then she was started on conservative management .
(Sod bicarb,Shelcal,Omeprazole,Iron folate)
Since then ,she is on routine followup with hemogram and serum creatinine levels,and her baseline creatinine levels were 3.2mg/dL.
In june 2022,she developed fever and productive cough associated with SOB for which CT chest was done,showing peripheral ground glass opacities,and septal thickening was noted
and few days later , she developed swelling of both lower limbs till the level of ankles,which were insidious in onset and gradually progressive
Then underwent dialysis for the first time through right IJV line,for 4 hours,and was on conservative management.
3 months later, she developed fluid filled bleb, on one finger and then over all the 10 fingers of hand in 10 days ,some of which ruptured on their own and some were pricked by the patient.
She developed eroding nails and distorted nails , hyperpigmented macules over the face and itching over the palms,and low grade fever associated with loss of apetite and alopecia.
Ulcers over palms , pulp of fingers associated with burning sensation
With autoimmune etiology suspicion, she was investigated further and was ANA profile and was tested Positive for Anti Ro 52and SSA/Ro 60++,and SSB/La+.
2days back she developed sudden onset developed movements of UL and lowerlimbs, for 3-4minutess, associated with blood from mouth,and there is a brief period of LOC .
similar episode one at 6:00 am, and then 2 similar episodes after they came here at 8:00am.
At presentation her blood pressure was 170/110 mmhg
inj lorazepam was given,
later leviteracetam and
when her seizures weren’t controlled then sodium valproate was given
She later then had continuous episodes of seizures lasting for more than 45 minutes .
In view of respiratory distress ( sats 60 ),and uncontrollable recurrent seizures she was sedated with IV MIDAZOLAM and intubated.
Post intubation, she had cardiac arrest ( no central pulses palpable ) 2 cycles of CPR done ROSC was achieved and post CPR monitor showed monomorphic VT and 2 times 200 J of DC shock was given and then it reverted to sinus tachycardia.
Course in hospital :-
After returning to normal rythm
Post cpr day 1 :- pt is on mechanical ventilator ACMV/VC mode with fio2 of 40 per peep :- 5 cms h20 tidal volume -450ml and t inspiratory -1.5 and started on iv antibiotics and patient is on sedation with midazolam cont iv infusion and her pupils are dilated and non reactive to light with dolls eye reflex: eyes moving on same side
And mri brain was done and it showed -? PRESS ? ODS ?uremic encephalopathy
Upper limb reflexes are present on left side and lower limb reflexes are absent and plantars are mute and derma referal was taken for the blebs over hand and was diagnosed as ?bullous phemphigoid ? Friction induced blisters and ophthalmology opinion was taken to rule out rasied icp but no raised ict features are seen on fundoscopy and nephrology opinion was taken i/v/o raised renal parameters and they advised for hemodyalsis and one session was done on 5/1/23 on next day midazolam infusion was stopped to plan for extubation but as patient is not taking breaths spontaneously extubation was not done and i/v/o raised pt aptt inr vit k was given and neurology opinion was taken and they advised for EEG and lumbar puncture was done and pulmonolgy opinion was taken for resuming ATT and advise followed and on D3 of intubation patient is on ACMV/Vc mode with rr :- 14cpm fio2 :-45 peep :- 5 VT :- 450ml tinsp :- 1.9 and she developed ulceration over the sacral region ? Bed sore and surgery opinion was taken and was diagnosed as having a soft tissue based non mobile and non blanchable ulcer with partial thickness skin loss and late superficial ulcer ? Grade 2 bed sore and reflexes of b/l UL and LL were absent and pupils decreased in size and reacting to lights and dolls eye moving to same side and GCS :- E1VTM1 and antifungal tab voricanzole was started (as BAL showed aspergillosis ) on day 4 of intubation pt was taken for second session of hemodialysis on 8/1/23 and anesthesia opinion was taken for weaning of from ventulator but as the weaning of criteria was not met and as patient is tachypnic patient is restarted on midazolam 30mg and fentanyl 200mcg as per anesthetist advise and patient is shifted to SIMV mode on day 5 of intubation sedation was stopped at 8:00 am as patient is taking spontaneous breaths and tracheostomy was done on 11/1/23 and another episode of dialysis was done on 13/1/23 and review mri scan was done on 13/1/23
MRI IMAGES:-




Interpretation:-

GENERAL EXAMINATION:-
Patient is in sedation.
She has hyperpigmentation on the face, upper limbs
Her nails


VITALS:
Temperature:afebrile
BP 160/110mmhg
Pulse 158bpm
RR 37 cpm
SYSTEMIC EXAMINATION
CVS : S1,S2 heard. No murmurs
RS
Ventilator :- ACMV /VC mode
CNS
Tone power not elicited
Reflexes :
B. T. S. K. A. P.
R. +. - - - - Mute
L. +. - - - - Mute
Investigations :-
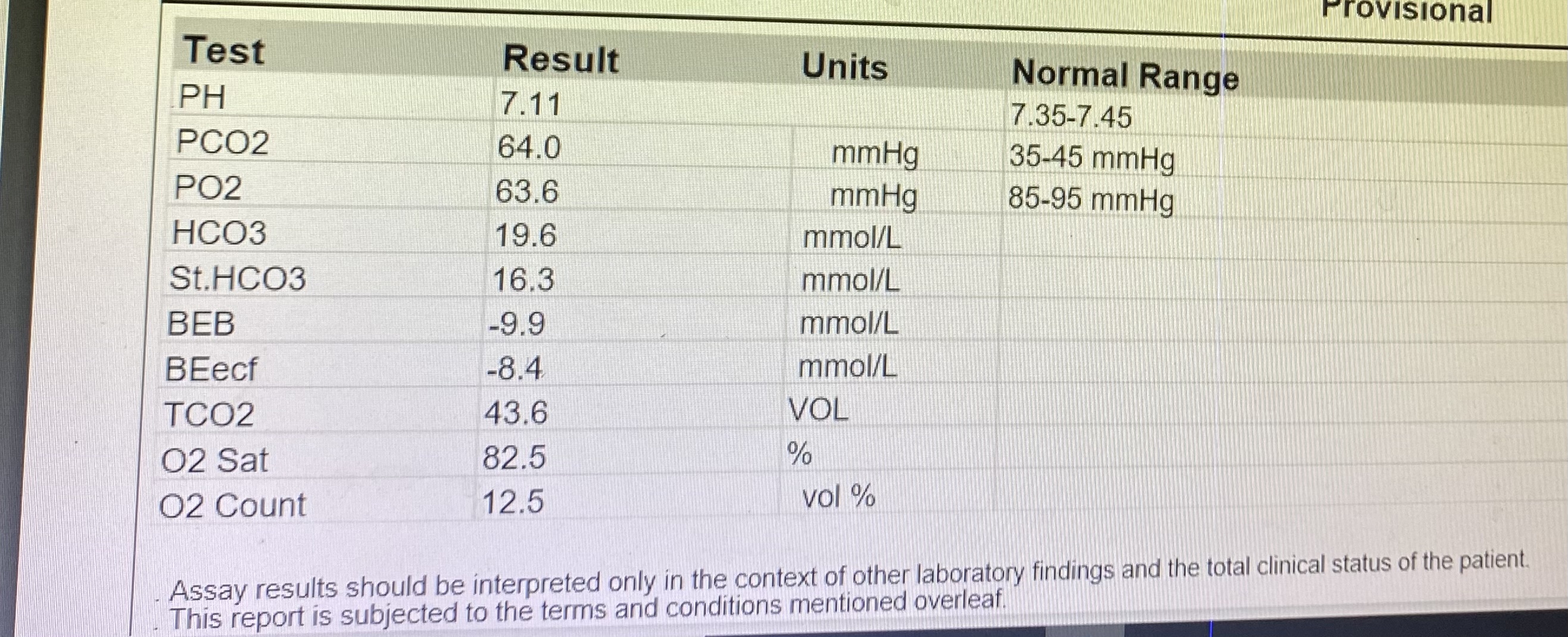
ABG TREND OF THE PATIENT:-
3/1/23






10/1/23




14/1/23











Provisional diagnosis:-
Generalised convulsive status epilepticus
Autoimmune vasculitis -PRES
AKI ON CKD _ STAGE V, With 2 SESSION of hemodialysis done (jun and dec) and 2 session of dialysis on 5/1/23 and 8/12/23
Pulmonary tb on ATT (since 20 days) with hemoptysis
Secondary to pulmonary tb anti synthase syndrome
(ANA2+, AntiRo52+),
Monorphic VT to sinus tachychardia tracheostomy with grade II bedsore
?anemia of chronic disease secondary to ckd
4ffps done on 11/1/23
Treatment:-
1. RT feeds 50 ml water with protein powder 2nd hrly , 100ml milk : 4th hrly, inj vancomycin 1gm/iv/bd in 100ml ns over 45 mins
- Inj pantop 40mg iv/od
- Inj zofer 4mg/iv/od
- Inj neomol 100ml /iv /sos
- Inj vit k 1 amp in 100 ml ns/iv/od
- Inj levipil 500mg in 100 ml ns /iv/bd
- Tab isoniazid(245mg) + rifampicin (490mg) + pyrazinamide(1225mg) + ethambutol(735mg)/rt/od
- Tab dolo 650mg /RT/ 6th hrly
- Tab Atorvas 20mg /po/H/s
- Syrup potklor 15ml/Rt/ tid
- Dvt stocking
- Airbed/waterbed
- Repeat abg 6th hourly
- Grbs charting 4th hourly
- E/D lubrex 0/0/0/0
- E/D moxiflox 0/0/0/0, both eyes 4times/ day
- Fudic cream L/A /bd/1week
- Zyte gel for L/A low lips
- Tab nodosis 500mg /po/bd
- Neosporin powder L/A for bed sore
- Rt upper end elevation
- Vitals monitoring 2nd hrly
- Grbs 4th hrly
- Tracheostomy care with suctioning every 2nd hrly
- Inj sodium bicarbonate infusion 50meq/slow iv/over 20 minutes /Stat



Comments
Post a Comment